
Stopping the bleed: a challenge for engineers
Did you know?
- First responders normally apply pressure to serious bleeding with a tourniquet on limb injuries or by packing gauze and pressing on injuries elsewhere
- This doesn’t work for all injuries, so engineers are developing ways to stem bleeding that include applying pressure directly to the wound from the inside
- These aim to keep patients alive until a surgical team can repair the damage to blood vessels or organs in hospital
Our story starts in a quiet commuter-belt town, just outside the M25. At first, Caleb* didn’t realise he’d been stabbed during a fight that almost ended his life. He didn’t see the knife, thinking he had merely been punched. Caleb only realised the extent of his injury when his friends pointed out the blood on his T-shirt. The knife had pierced his lower abdomen, cutting the iliac artery, a major artery deep in the pelvis.
Thirty minutes after the 999 call, the air ambulance arrived. Another half an hour later they arrived at the major trauma centre. By this time, they had used up the stock of blood carried on the helicopter. On arrival in hospital, Caleb went straight into surgery. Saving Caleb’s life took three anaesthetists and four surgeons, and then 22 days of intensive care and two further operations. He was discharged from hospital five weeks to the day from the attack.
Every wound is different
The variety of non-compressible haemorrhage
Human anatomy is complex. NCH can result from injury to the torso – anywhere in the abdomen, chest or pelvis – and where it joins the arms, legs and neck. The bleeding might come from a large vessel, such as the aorta that joins the heart, or from several smaller vessels in an organ, such as the liver. Unlike compressible haemorrhage, it may be difficult to locate NCH.
This is especially true in blunt-force trauma, where there may be no open wound. Such injuries in the torso can be particularly lethal. The median time to death in soldiers injured in the torso is about 30 minutes.
Trauma is not the only cause of NCH. Severe bleeding as a complication of childbirth causes a quarter of maternal deaths. It can also be psychologically traumatic – another reason to develop new solutions to NCH. External aortic compression devices, which press on the aorta to stop blood flow, can help medical staff treat haemorrhage.
Caleb can’t remember much about his assault. 40% of his blood volume – some two litres – bled into his abdominal cavity and the tissues around his iliac artery. The prolonged period of low blood pressure, known as haemorrhagic shock, caused permanent changes to Caleb’s cognition. He never resumed his degree studies. If the initial haemorrhage-control surgery had been delayed, even by a few minutes, he wouldn’t have survived. The continued blood loss would have induced cardiac arrest, from which the chances of recovery are close to zero.
The situation would have been much simpler if the knife had wounded a limb. The first responders could have limited the bleeding with a tourniquet, a relatively simple device that applies pressure to stop blood flow. Unfortunately, in Caleb’s case, the haemorrhage was ‘non-compressible’: applying external pressure would not stop the bleeding.

US Army medics in training to apply tourniquets, which prevent haemorrhage by stopping blood flow to limbs © Alamy
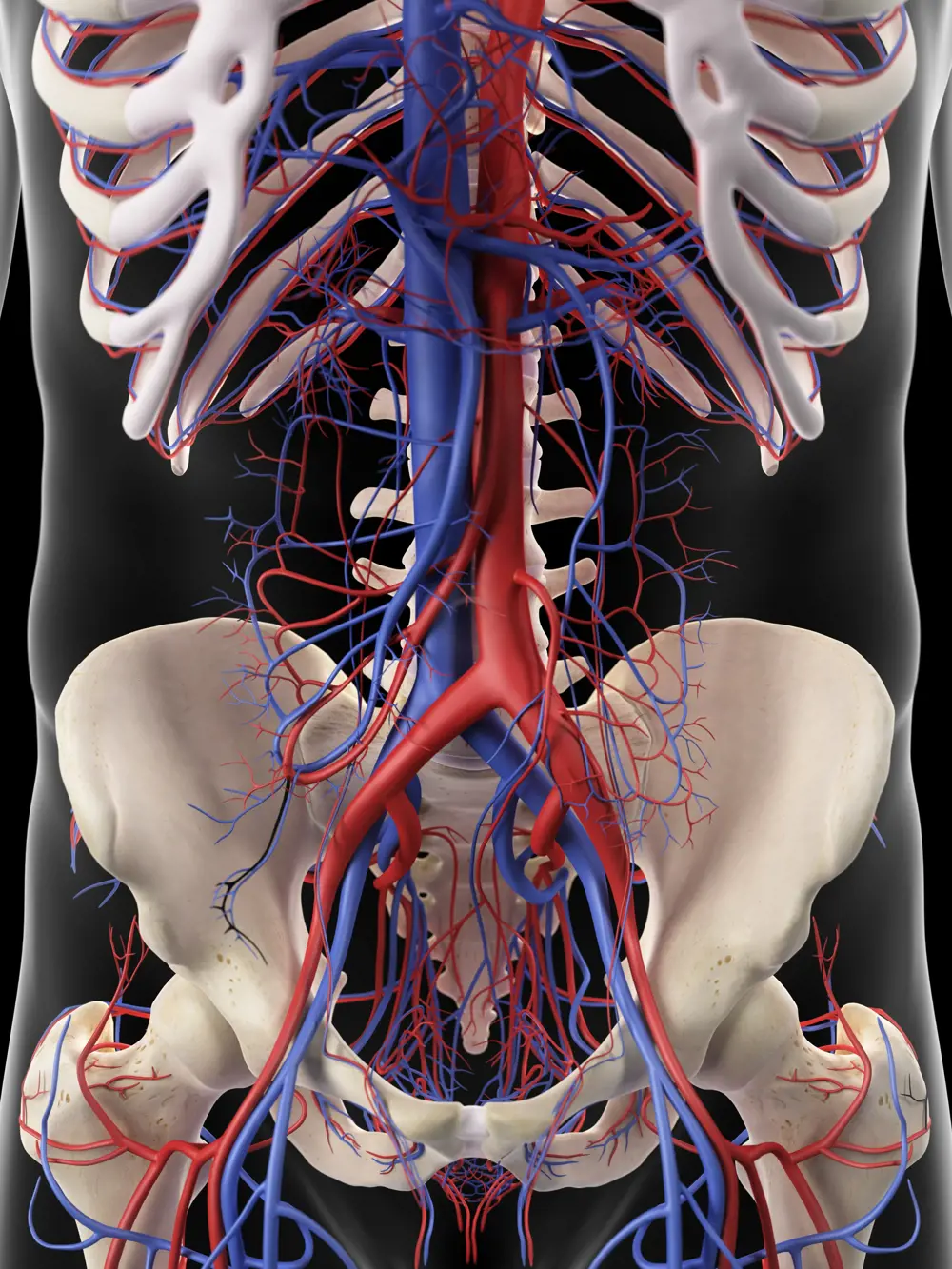
The aorta carries blood from the heart to major blood vessels, such as the iliac and femoral arteries to the lower limbs, and the arteries supplying vital internal organs such as the liver, spleen and kidneys. When cut or torn, vessels in this dense network are very difficult or impossible to compress compared to those in the limbs © Shutterstock
Bridging the gap to hospital
“Non-compressible haemorrhage patients who make it alive to hospital will almost always survive, with the sophisticated surgery and resuscitation strategies available to us,” says Professor Nigel Tai, a British Army trauma surgeon who also looks after patients in London. Typically, the greatest risk to life is on the street or on the way to hospital. In conflicts, this is on the battlefield, before evacuation. “We call these deaths ‘preventable’,” says Tai. If medics can keep patients alive until they reach a hospital then surgical teams can stop the bleeding, repair damaged blood vessels and pack injured organs.
In recent years, surgeons have relied on blood transfusions and drugs that support clotting before getting to the operating theatre – but these techniques can’t stem catastrophic bleeding. New devices are needed to plug holes and seal off bleeding tissues that would normally only be accessible via a surgeon’s incision.
🪡 A needle in a haystack
Identifying the source of the injury
Non-compressible haemorrhage within the human torso can have many sources that may be difficult to identify, such as:
- organs (for example the lungs, liver and spleen) causing bleeding into a body cavity
- blood vessels, including arteries such as the aorta, and large veins. These can be in body cavities or at junctions, such as the neck, groin or shoulder
- pelvic bones
- direct bleeding from hundreds of small blood vessels, which tear as the bone breaks
- indirect trauma to large nearby pelvic vessels torn by the fractured ends
of bone.
A complicating factor is the sheer number of different types of non-compressible haemorrhage (NCH) – among them, bleeding from stab wounds such as Caleb’s, to severe bleeding after childbirth.
Because such different anatomies are involved, no single device will work for all injuries. “This has led to an innovation gap,” says Tai, “and a need for new thinking.” Until recently, researchers focused on a conceptually easier approach, developing new ways of replacing lost blood, instead of stemming blood loss in the first place. Tai firmly believes we need engineers’ skills to solve the issue.
Time is life
If you’ve ever seen 127 Hours, Saving Private Ryan, or Band of Brothers, the tourniquet takes a starring role. Tourniquets wrapped tightly around the limb can apply enough pressure to stop blood flowing into the vessel. These simple medical devices are very successful in managing bleeding from the limbs.
However, tourniquets are “useless” in managing non-compressible bleeding, explains Surgeon Commander Pippa Bennett, a Royal Navy trauma surgeon at the Oxford Trauma Service. Take the junctions between the torso and legs, arm, and neck. It’s clearly inadvisable to apply a tourniquet at the neck, and there’s not enough purchase at the groin or shoulder – it’s difficult to apply enough local pressure when a bleed is deep within a body or behind a bone.
The only current solution is ligation with a suture, tying a thread or wire around the vessel to close it off. “Where time is life, the time to an operating theatre could be the difference between life and death. We need something in between,” says Bennett.
There is a critical technology void between tourniquets and surgery, where engineering approaches could address the problems. These approaches must consider the armpits, groin, abdomen, pelvis, and long bones such as the arms and legs. New devices may need to be based around a thorough understanding of how a complex, flowing fluid such as blood, containing multiple different cell types and component fluids, behaves in injured, leaking blood vessels. Equally, the material properties of injured tissues, and the interface between them and any new device must also be accounted for. The problems may appear complex, but solutions could involve simple adaptions or exploitations.
🪂 Anatomy of a fall
A NCH case study
A 41-year-old military parachutist sustained severe injuries when his parachute failed to deploy. Paramedics on the scene realised that he had life-threatening internal bleeding. At first they couldn’t see where it was coming from. His leg was deformed, suggesting he had fractured his thigh bone. He complained of pain in his abdomen before falling unconscious. In hospital, he was given blood transfusions as well as blood components to help him form blood clots.
But when he was rushed to theatre, there was minimal blood in his abdomen. Instead, multiple complex fractures of his pelvis, hip socket and thigh bone had caused catastrophic bleeding. This NCH could only be treated by roughly realigning the bones and reducing the dead space into which blood was collecting. The patient was given more blood and clotting agents and, over a week, underwent more than 24 hours of operating to fix his bones.
Cases like Caleb’s demonstrate one of the key challenges with managing NCH: detection. In many cases, the clinician cannot diagnose it in time to save the patient. Early detection is critical. It is easy in patients with large visible wounds and significant bleeding. Injuries to the solid organs in the abdomen or pelvis or long bones can cause significant blood loss that can take time to identify.
This isn’t easy to detect outside of hospitals, where CT scanners can take cross-sections of the body and pinpoint injury. Thanks to improved clinical training, clinicians now have better ‘spider senses’, attuned to significant internal bleeding. But this can go only so far. Handheld ultrasound, where available, may detect blood in the chest or around the intestines but can’t detect blood in the tissues at the back of the abdomen that anchor the major abdominal blood vessels.
Balloons, foams and AI-guided ultrasound
Since the 2010s, the medical toolkit has expanded beyond manual pressure and tourniquets to several early-stage devices.
Air ambulances in the UK and Norway have trialled the snappily named resuscitative endovascular balloon occlusion of the aorta. REBOA, for short, is designed to treat haemorrhages to the abdomen or pelvis. The ‘balloon’ itself is small, with a working volume of about eight millilitres when inflated. It is attached to a long tube or catheter.
Getting the balloon in place involves inserting the tube and empty balloon into the femoral artery in the upper thigh and threading it about 45 centimetres to the aorta. Once in place, inflating the balloon drastically reduces blood flow beneath it, meaning that less blood leaks out from the injured tissues.
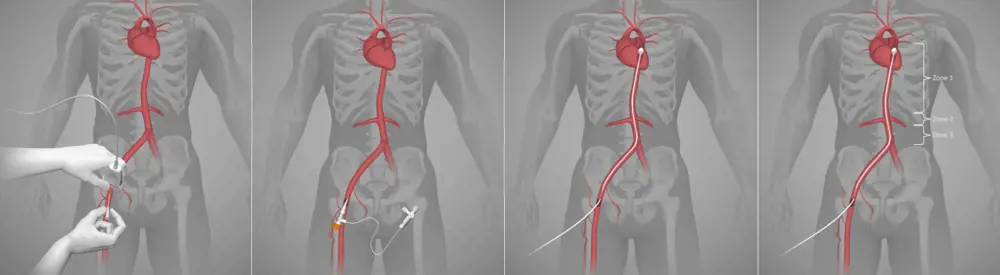
REBOA is inserted through the femoral artery, threaded to the aorta and inflated © Image permission kindly granted by the authors of the paper ‘REBOARREST, resuscitative endovascular balloon occlusion of the aorta in non-traumatic out-of-hospital cardiac arrest: a study protocol for a randomised, parallel group, clinical multicentre trial’, Brede et al, Trials, 2021
REBOA requires a skilled clinician, and often access to imaging tools. The evidence around benefit is mixed. In 2023, a UK clinical trial found that patients receiving REBOA in the emergency department were slightly more likely to die than patients who didn’t receive it. This was surprising as other (albeit unrandomised) studies done in the US have shown that REBOA helps survival. Some have concluded that the poor results in the UK trial were likely down to the delay in getting patients into theatre and other nontechnical factors.
Researchers at MIT are working on a handheld ultrasound device that uses AI and robotics to get the tube to the femoral artery more easily. One researcher behind the device likens it to “an intelligent stud-finder married to a precision nail gun”. A startup company, AutonomUS Medical Technologies, is working on getting the device regulatory clearance.
Researchers at MIT are working on a handheld ultrasound device that uses AI and robotics to get the tube to the femoral artery more easily. One researcher behind the device likens it to “an intelligent stud-finder married to a precision nail gun”.
Another consideration is REBOA’s potential side effects. The aorta carries blood to the kidneys, intestine and lower limbs. Blocking it can have fatal consequences. To address this, clinicians are also testing a twist on REBOA, P-REBOA, where the balloon is only partially inflated. This trade-off allows some blood flow to sustain organs, but it raises the risk of haemorrhage compared to the fully inflated balloon.
ResQFoam is another strategy designed to stop bleeding into the abdominal cavity. It’s delivered as two liquids squirted simultaneously into the cavity, where they mix and expand as a foam, filling the space surrounding the organs. The foam stops bleeding by exerting pressure on the bleeding structures and tissues inside, until it solidifies and is later removed during surgery.
So far, ResQFoam has only been tested on animals, but clinical trials are on the horizon in trauma centres in the US. These will test how safe and effective the foam is in treating patients who have lost more than 30% of their blood volume, or about 1.5 litres.

ACT Medical’s device to treat stab wounds, before and after activation © ACT Medical
After two of his friends were stabbed in London, Joseph Bentley wanted to find a way to help first responders treat knife wounds. A final-year product design student at Loughborough University at the time, Bentley developed a Dyson Award-winning prototype and received an Enterprise Fellowship from the Royal Academy of Engineering to support its development. Today, he leads ACT Medical, a startup company that has commercialised the device.
Stab wounds tend to be deep and narrow penetrating injuries. Medics ordinarily pack these with gauze and blood clotting agents to staunch blood flow. However, once in hospital, the gauze is hard to remove without tearing out blood clots, causing bleeding.
ACT Medical’s device, the balloon occlusive barrier (BOB), works in a similar way to the REBOA and ResQFoam, although its mechanism is very different. While BOB’s composition is a trade secret, Bentley explains that it is effectively an engineered sponge that uses manually stored energy to expand once activated, acting like a spring to deliver pressure to the inside of the wound.

The ACT Medical team. (Clockwise from left) Joseph Bentley, Nicky Johnson, Nathan Wenban and Emma Priestley © ACT Medical
When inserted into the wound, the sponge expands, applying enough internal pressure to stop bleeding. According to ACT Medical’s tests, it takes three minutes to control the bleeding. The device stays there, buying the patient time, until theatre, when it is deflated and removed. Unlike the gauze, the blood clot stays intact. “I often say it’s like the balloon on the inside of a papier mâché,” says Bentley.
Last summer, the team successfully conducted preclinical trials. The team hopes to have regulatory approval for the device in just over a year for wounds to limbs and junctional regions such as the groin or shoulder.
Engineers, take note
The fact that these approaches to trauma relief have been developed in the past 15 years is a testament to the ingenuity of trauma specialists, engineers and designers. “This type of problem-solving invention shows the significant impact engineers can have on serious global issues and is why I created the James Dyson Award,” said Sir James Dyson FREng FRS, on presenting his international award to Bentley in 2021. The innovation demonstrates the value in bringing fresh perspectives to generating new approaches to this condition.
The story doesn’t end there. As Bentley puts it, “no two wounds are the same.” None of these solutions is a silver bullet. Each type of NCH may need a different solution, tailored to a specific body part. Medics treating someone with multiple types of NCH may need a toolkit of different devices and solutions to buy them enough time and get them to the operating theatre. It’s not just the wound that affects the solution. Some environments, such as a poorly lit roadside or a battlefield with uneven terrain, are more challenging than others. This could make a real difference in conflicts such as Ukraine or Gaza, where bleeding from wounds from gunshots, shrapnel and explosions is the main cause of death.
“What surgeons may see as a problem of anatomy, engineers may see as an opportunity to rework solutions from nonclinical areas such as hydraulics, civil engineering and materials science,” explains Tai.
All of this underlines the need for engineers’ unique skills. “What surgeons may see as a problem of anatomy, engineers may see as an opportunity to rework solutions from nonclinical areas such as hydraulics, civil engineering and materials science,” explains Tai. “These are the new perspectives this space is crying out for.”
Caleb’s story is not unique. It is one of many young people in the UK and globally who are the victims of non-compressible bleeding. Caleb was one of the lucky ones, his injury happened in a country with a well-developed prehospital care system and trained medics. Many aren’t so lucky; their country lacks the infrastructure or the capacity to quickly move patients to hospital. By developing new approaches that can buy time, we can improve their chance of surviving to hospital.
*Names and narrative details have been changed.
Contributors
Colonel Nigel Tai is a British Army Trauma and Vascular Surgeon who is a consultant at the Royal London Hospital Major Trauma Centre. He leads the UK Defence Medical Services (DMS) Non-Compressible Haemorrhage working group. Col Tai is the DMS Professor of Military Surgery and an honorary Professor of Trauma Surgery & Innovation at Queen Mary University of London.
Rob Staruch is a military specialist trainee in burns, plastic and reconstructive surgery based in Oxford. After attending Harvard University as a Fulbright Scholar, he gained a PhD from the University of Oxford in 2023 on the effects of primary shock waves from explosive blast on skeletal muscle. His interests lie in engaging engineers in critical defence healthcare problems.
Surgeon Commander Pippa Bennett is a consultant orthopaedic trauma surgeon in the Royal Navy working at the John Radcliffe major trauma centre in Oxford. She has a specialist interest in fractures involving the pelvis and acetabulum.
Joseph Bentley is an internationally award-winning Product Designer from Cambridge UK, holding enterprise fellowships with the Royal Academy of Engineering and Royal Society for Arts. Joseph graduated best in class in Product Design BSc from Loughborough University, winning the Vice Chancellor’s award for excellence, and has prior work experience as a Medical Designer at TTP plc.
Keep up-to-date with Ingenia for free
SubscribeRelated content
Health & medical
A gamechanger in retinal scanning
2006 MacRobert Award winner Optos rapidly became a leading medical technology company and its scanners have taken millions of retinal images worldwide. There is even a display at the Science Museum featuring the Optos development. Alastair Atkinson, of the award-winning team, describes the personal tragedy that was the trigger for the creation of Optos.

Kidney dialysis
Small haemodialysis machines have been developed that will allow more people to treat themselves at home. The SC+ system that has been developed is lighter, smaller and easier to use than existing machines.

Engineering polymath wins major award
The 2015 Queen Elizabeth Prize for Engineering has been awarded to the ground-breaking chemical engineer Dr Robert Langer FREng for his revolutionary advances and leadership in engineering at the interface between chemistry and medicine.
Blast mitigation and injury treatment
The Royal British Legion Centre for Blast Injury Studies is a world-renowned research facility based at Imperial College London. Its director, Professor Anthony Bull FREng, explains how a multidisciplinary team is helping protect, treat and rehabilitate people who are exposed to explosive forces.
Other content from Ingenia
Quick read

- Environment & sustainability
- Opinion
A young engineer’s perspective on the good, the bad and the ugly of COP27

- Environment & sustainability
- Issue 95
How do we pay for net zero technologies?
Quick read

- Transport
- Mechanical
- How I got here
Electrifying trains and STEMAZING outreach

- Civil & structural
- Environment & sustainability
- Issue 95