
How robotics can improve retinal surgery
Did you know?
All about eyes 👀
- Age-related macular degeneration (AMD) is the leading cause of blindness worldwide and is expected to affect 288 million people by 2040
- A 2018 trial placed patches of stem cells on the retinas of patients with AMD, with the patients able to read again after a few months
- Advances in microrobotics have led to development of a robotically assisted instrument that can place the stem cells with more precision
Robotics are increasingly being used in healthcare settings and the benefits of robotic assistance in performing surgery are easy to understand. Robots can offer enhanced dexterity, better control of instruments (by, for example, the avoidance of tremor), greater precision, and, through the use of a camera inside the patient’s body, a clearer view of the operating site. However, although explored in many branches of surgery, the use of surgical robots is not widespread – and some 70% of the million and a half robotically assisted procedures worldwide are performed in the US. Even in prostate surgery and orthopaedic joint replacement, in which they are most commonly used, they still account only for a minority of operations.
Robots can offer enhanced dexterity, better control of instruments (by, for example, the avoidance of tremor), greater precision, and, through the use of a camera inside the patient’s body, a clearer view of the operating site.
Robots are particularly valuable in procedures that are intricate and small scale, which is one of the main reasons that they are used in prostate surgery. The use of robots to operate at the truly microscopic level is still in its infancy. Unsurprisingly, ophthalmology is at the forefront of this endeavour, as few of the body’s most critical anatomical structures are as complex and delicate as the retina.

The figure illustrates key components of the eye anatomy. The retina is the element that is responsible for capturing light, and creating the electrical signals that are sent to the brain. The retina is a layered structure, and different diseases affected its different layers © Shutterstock
❓ What's age-related macular degeneration? And how is it treated?
How stem cells can help age-related macular degeneration
AMD is the most common cause of vision loss in older people. The condition results from the degeneration of the retinal pigment epithelium, one of the constituent layers of the retina, which is the light-sensing tissue that lines the interior of the eye. The macula area of the retina is responsible for the sharp and detailed images at the centre of our visual field, and tissue degeneration here leads to the severe blurring that characterises AMD. Reading, driving and recognising faces or details of any kind become progressively more difficult.
AMD is categorised as ‘wet’ – resulting from the growth of abnormal blood vessels at the back of the eye – or ‘dry’ – caused by a build-up of fatty deposits within the retina. Drug injections or other treatments designed to inhibit the growth of the blood vessels can often prevent wet AMD from worsening. Dry AMD can be alleviated with a vision aid.
One of the main non-drug treatments for wet AMD relies on administering a light-activated chemical agent and then shining a beam of light on to the troublesome blood vessels. Once activated, the chemical destroys the sensitised vessels. An alternative is to destroy the abnormal vessels using a laser beam. However, neither method is suitable for every patient nor guaranteed to work. Hence the interest in stem cells, which could, in theory, prove valuable in treating a lengthy list of medical conditions, including both types of AMD.
In 2018, vitreoretinal surgeon Professor Lyndon da Cruz of Moorfields Eye Hospital and Professor Peter Coffey of the UCL Institute of Ophthalmology reported their success at introducing retinal pigment epithelium (RPE) stem cells into the retinas of AMD patients. In the laboratory, they first grew single layers of stem cell derived RPE cells on synthetic membranes. When the cells were ready to use, they cut out small 6x3mm ‘patches’ of membrane that they could pick up and handle using a specially designed surgical tool. They were able to use this tool to slide the patch between the layers of the retina in the region affected by the AMD. The new RPE cells integrated with the patients’ own cells and began functioning. Within months, both patients were able to start reading again.
With the aid of an operating microscope, eye surgeons have extensive experience in performing intricate procedures – and not only on the visible outer parts of the eye, but also its deeper structures including the retina. However, as in other branches of medicine their ambitions keep on advancing. Among recent advances is an intention to treat potentially blinding diseases such as AMD using stem cells. These cells have the potential to give rise to a population of any of the many cell types that exist in the body, including those found in the retina and directly responsible for vision. Recent experimental surgery has already demonstrated the feasibility of using stem cells in the eye.
A first clinical trial of the procedure involved placing ‘patches’ of stem cells [see ‘❓ What's age-related macular degeneration? And how is it treated?’] towards the back of the patient’s eye, and just below the diseased area of the retina. The trial has seen positive results – but enhancing the surgical precision should boost efficiency and improve outcomes. Ideally, surgeons should be able to inject stem cells precisely where they are needed within the various layers of the retina, some of which are as thin as 10 to 20 μm: less than the width of a human hair.
Today’s microscopy already allows surgeons clear sight of the back of the eye. But for future possible operations, even the best view of the area to be treated is not, by itself, enough. The operating procedures involved demand a steadiness and delicacy that even the most skilful hands would find it hard to achieve. The biology of creating and using stem cells has run ahead of the technology required to make the best use of them. Hence the need for the assistance of a robot.
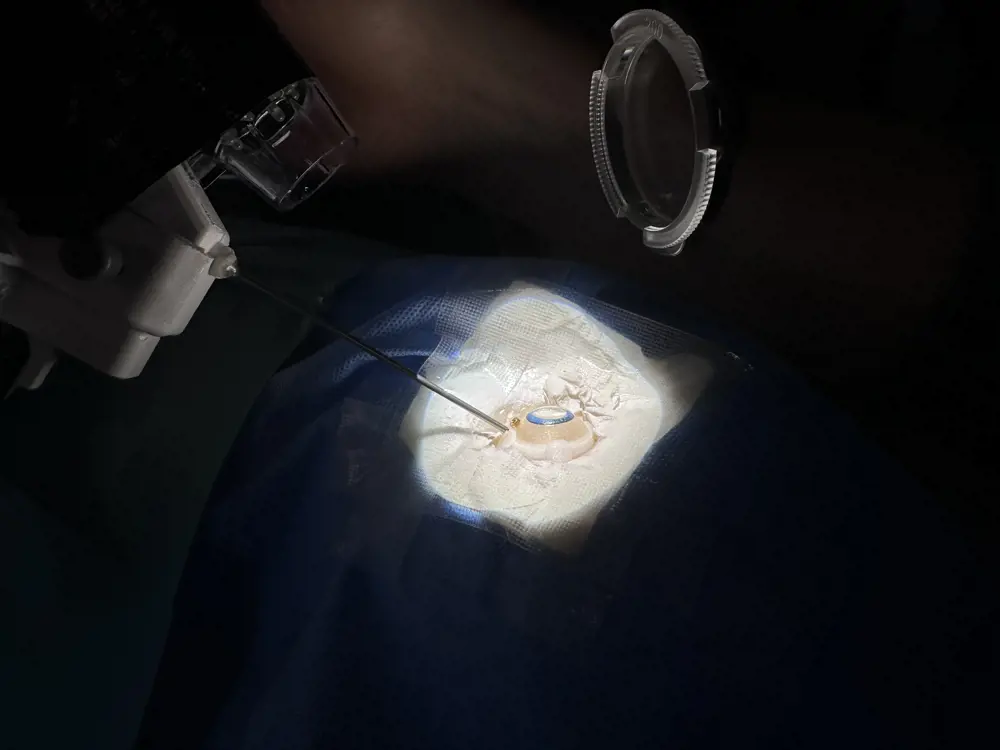
Close up of the experimental setup illustrated in the next figure. A phantom eye with dimensions and appearance similar to a human eye is used for evaluation. The surgical tool is approaching the eye to be inserted through a trocar (orange insert)
Developing robots with enhanced precision
Robots already feature in some surgical operations, but most of these procedures rely on the use of rigid instruments. Engineer Christos Bergeles is Professor of Surgical Robotics at King’s College London where his work is partly funded by the National Institute for Health Research. In collaboration with ophthalmic surgeon Professor Lyndon da Cruz, he is aiming to add greater precision and flexibility to robotic microsurgery. As Bergeles points out, when aiming to work within the layers of a tissue as thin as those of the retina, instruments must take a tangential approach to their target: one in which the tips of the instruments can move towards the tissue surface at a slight angle. This allows the instruments not only to penetrate the retina but slip between its layers. So how to achieve such an approach when the target tissue is the inner lining of a sphere, and the surgeon is using instruments that have entered the eye by being pushed through its outer wall? Bergeles’s answer might be summarised as relying on a needle comprising ‘tubes-within-tubes’. Using this approach he has been able to achieve the snake-like flexibility required to create a needled instrument with a tip that can be pointed in any direction.
The needle used by his robot comprises several fine, concentric metal tubes with a shape memory of a simple curve. To penetrate the tough outer layer of the eye – its white or sclera – the surgeon first uses a conventional circular cutting tool to make a small hole. They then move the robot, which has a short, narrow and rigid tube on the end of its arm, to the newly created opening. Once its tip has entered the jelly-like fluid, or vitreous, that fills the interior of the eyeball, a short length of the first of the nested tubes emerges and forms itself into a curve. From this tube emerges the next of the group and from it, in turn, the narrowest of the tubes. Each of these assumes its own, ‘memorised’ curve, with the outer end of the narrowest serving as the tip of the needle.
At this stage the tip’s orientation will depend on the curvature of the three tubes. The robot’s operators can then lengthen or shorten each tube and rotate each one independently of the others. This alters the position and movement of the tubes: in effect steering them and allowing the operator to move the needle tip as needed before sliding it into the retina at a chosen point. The outer diameter of the widest tube is some 800 μm; the narrowest, forming the needle’s tip, is just 160 μm.
As Bergeles explains, while it might be tempting to consider simply injecting the required stem cells at one particular location in the hope that they will then diffuse through the retinal tissue to where they are needed, this doesn’t work. Instead, the surgeon will have to slowly introduce the stem cells successively in tiny, microlitre volumes of fluid, each containing perhaps a few thousand cells. Each injection may take up to a couple of minutes before the needle is withdrawn from the retina and reinserted in one of several nearby locations covering a chosen region. For an unaided human operator, this task would require extraordinary powers of concentration, dexterity, and physical control; it will still need considerable skill, even with the aid of a robot that can compensate for factors such as hand tremor.

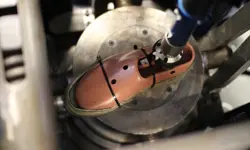
The developed robotic system, showcased within the mock operating room of the Department of Surgical and Interventional Engineering at King’s College London © Courtesy of China Global TV Network

Illustration of potential system draping, so that it can enter the sterile zone of an operating room
How to control the robot
Surgeons will use a console of some kind to advance and retract the needle, and to steer it in three dimensions. The distances moved by the surgeon’s hands will be scaled down to allow for the tiny movements needed to correctly align the needle inside the eye, slide it into the tissue, and introduce the cells. Bergeles is aiming for a resolution of just a few microns.
To give the surgeon a clear view of the back of the eye, a light source illuminates its interior, having been introduced through another small slit in the sclera. The operating site will then be visualised in the normal way through the patient’s dilated pupil. Bergeles hopes that this will eventually be supplemented by optical coherence tomography, a non-invasive technique that offers a real-time, cross-sectional view of the retina. This could reassure surgeons that the infused stems cells are being deposited in the correction location.
The electric motors and the associated gearing that move and rotate each of the instrument’s concentric tubes are housed in a container mounted on a firm robotic arm with three directional mobility. This moves the robot towards the patient’s head and aligns it with whichever eye is to be treated. The robot then carefully moves forward to bring the short rigid tube projecting from its front surface into contact with the small hole already made in the outer wall of the patient’s eyeball, through which the needle enters.
Although Bergeles has focused his attention on AMD, an instrument offering such precision and flexibility could be widely applied to treat other eye diseases. As well as using different stem cells to treat other retinal conditions, it could be used to deploy other therapeutic agents that need precise placement, such as gene therapy for example. So far, Bergeles has tested the technique on cadaver pig eyes and on the plastic model eyes that ophthalmic surgeons use in training. Bergeles and da Cruz hope to start preliminary human trials in a few years. In the meantime, their group is investigating various commercialisation opportunities.
The benefits of a robotic approach will not only make existing eye operations safer and more effective but, as in the work of Bergeles and de Cruz, offer the possibility of new procedures that would otherwise be virtually impossible.
Contributors
Geoff Watts
Author
Christos Bergeles is Professor of Surgical Robotics at King’s College London where he leads the Robotics and Vision in Medicine Laboratory based at St Thomas’s Hospital. He has previously worked in the Hamlyn Centre for Robotic Surgery at Imperial College London, and the Department of Medical Physics and Biomedical Engineering at University College London.
Keep up-to-date with Ingenia for free
SubscribeRelated content
Health & medical
A gamechanger in retinal scanning
2006 MacRobert Award winner Optos rapidly became a leading medical technology company and its scanners have taken millions of retinal images worldwide. There is even a display at the Science Museum featuring the Optos development. Alastair Atkinson, of the award-winning team, describes the personal tragedy that was the trigger for the creation of Optos.

Kidney dialysis
Small haemodialysis machines have been developed that will allow more people to treat themselves at home. The SC+ system that has been developed is lighter, smaller and easier to use than existing machines.

Engineering polymath wins major award
The 2015 Queen Elizabeth Prize for Engineering has been awarded to the ground-breaking chemical engineer Dr Robert Langer FREng for his revolutionary advances and leadership in engineering at the interface between chemistry and medicine.
Blast mitigation and injury treatment
The Royal British Legion Centre for Blast Injury Studies is a world-renowned research facility based at Imperial College London. Its director, Professor Anthony Bull FREng, explains how a multidisciplinary team is helping protect, treat and rehabilitate people who are exposed to explosive forces.
Other content from Ingenia
Quick read

- Environment & sustainability
- Opinion
A young engineer’s perspective on the good, the bad and the ugly of COP27

- Environment & sustainability
- Issue 95
How do we pay for net zero technologies?
Quick read

- Transport
- Mechanical
- How I got here
Electrifying trains and STEMAZING outreach

- Civil & structural
- Environment & sustainability
- Issue 95